


In the early years of dental sleep medicine, Dr. Keith Thornton had a big idea: Patients who use snoring and sleep apnea appliances should be given the tools to manage their own condition, with guidance from their dentist.
Snoring is one of the most common symptoms of obstructive sleep apnea (OSA), a condition that arises when the tissues of the airway relax and completely stop airflow despite the patient’s breathing effort. Tone is restored when the patient gasps awake. OSA is associated with heart disease, stroke, diabetes and early death.
An estimated 9% of women and 24% of men have sleep apnea. Unfortunately, the preferred sleep apnea treatment — a continuous positive airway pressure (CPAP) mask — is known to have low adherence, even though the mask is effective if worn properly. Oral appliances, on the other hand, are known to have high adherence, with one study showing oral appliances to be well accepted by 90% of patients. All these factors create a big opportunity for dentists to step up and rescue their patients.
Dr. Thornton’s simple philosophy transformed the practice of sleep apnea therapy in the dental office. There are clinicians who do not believe that patients have the skill or the training to manage their condition. One risk often cited by dentists is that the patient could over-titrate the appliance, causing pain, tooth movement and liability for the dentist. However, with proper guidance from the dentist, patients can easily self-titrate their appliance to the optimal treatment position. This reduces time-intensive and inconvenient appointments.
TAP® Position in the Dental Literature
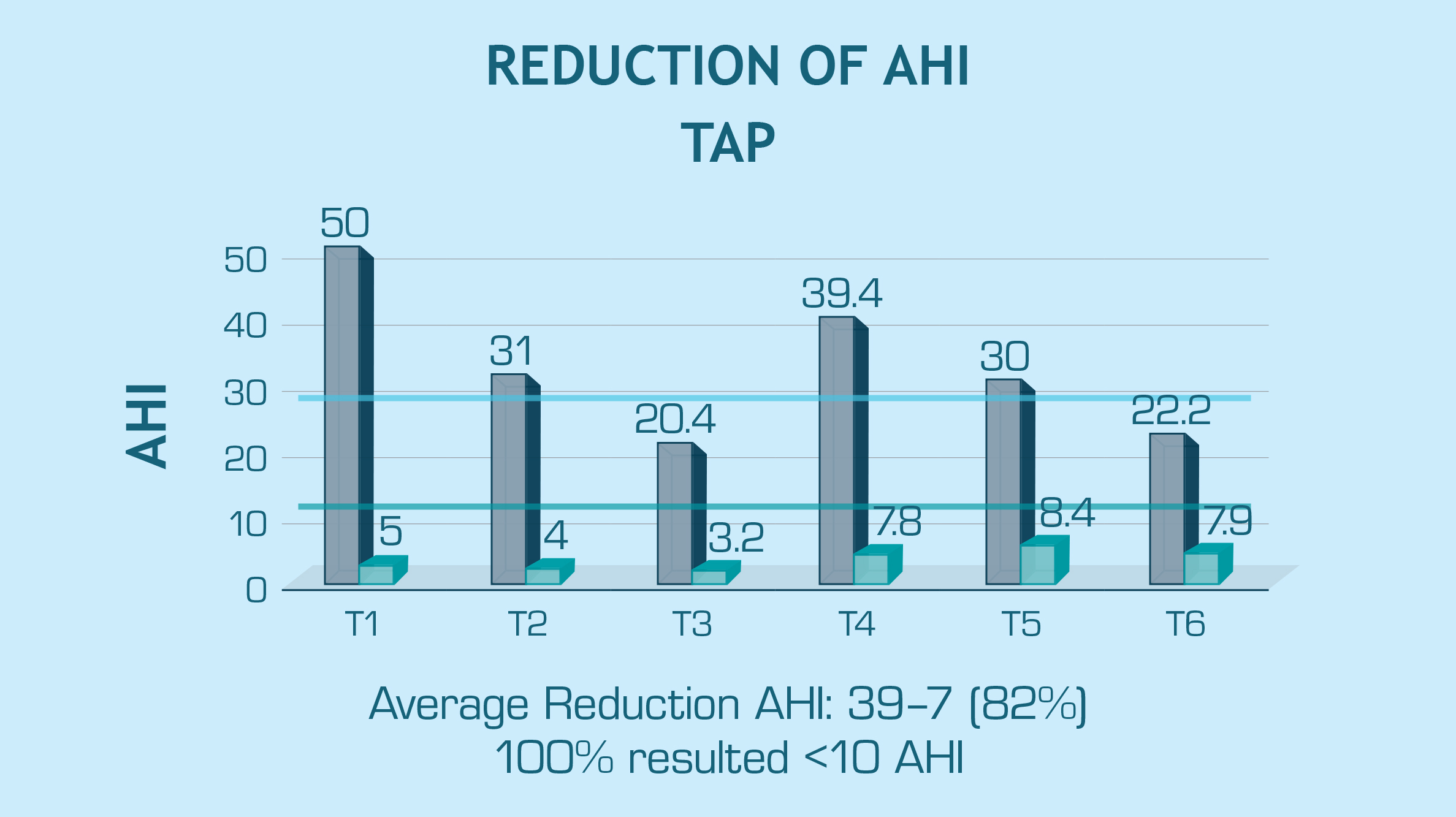
Research was clearly needed to evaluate the effect of self-titration on key sleep metrics like apnea-hypopnea index (AHI), which is used by sleep physicians and insurance companies to measure severity of disease. The success threshold with an oral appliance for OSA is an AHI reduction greater than 50% and an AHI less than 10.
A study by Hoekema et al. in a group of severe patients showed that the TAP® appliance achieved a reduction of AHI from 39 to 7.8 (80%) and was equal to CPAP. A seminal study by the Army of 497 patients showed a reduction from 30 to eight. All the studies on the TAP (total of six) referenced in the American Academy of Sleep Medicine (AASM) clinical guidelines achieved the definition of success of a reduction in AHI of at least 50% and below 10.
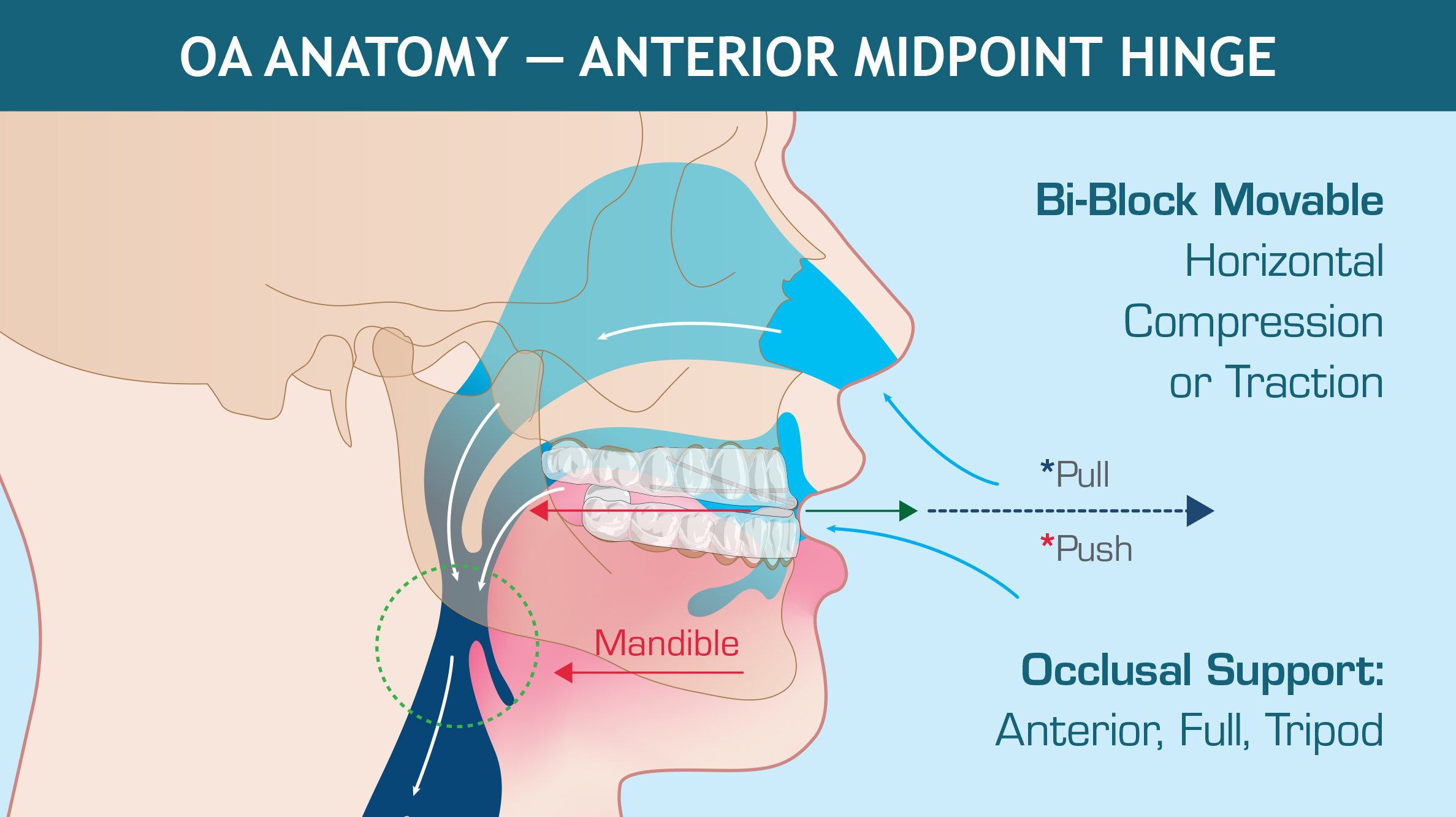
The key to this success is the TAP single-point midline titration capability, which enables titration beyond the patient’s natural bite range (when necessary).
The Thornton Adjustable Positioner (TAP) sleep care system was launched in the early 1990s, when sleep apnea treatment was in its infancy. Since then, over 100 different nightguards have been introduced to treat snoring and sleep apnea. For the most part, these appliances are in the mandibular advancement device (MAD) category. The design usually involves the upper and lower tray joined or connected in some way to allow the dentist to position the jaw forward in relation to the mandible while the patient is asleep. Optimal positioning of the jaw activates the muscles and ligaments of the upper airway, preventing them from collapsing and vibrating — thereby preventing the snoring sound.
How Do Patients Titrate the TAP Appliance?
The treatment strategy that Dr. Thornton developed was based on the understanding that the tone of the airway tissues changes in response to many different factors, such as inflammation, cold or flu symptoms, humidity in the air, weight gain, and alcohol or drug use. It is for these reasons that patients require a simple method to fine-tune their jaw position based on three high-level criteria:
- Has the snoring returned or worsened?
- Has sleep quality changed?
- Is the jaw position painful?
As MADs are delivered in the dental office while the patient is awake and seated, it can be difficult to find a therapeutic jaw position. The dentist can only assess the fit, form and function of the snoring and sleep apnea appliance like any other nightguard. At best, the established jaw position is an educated guess based on clinical experience.
Dr. Marc Raphaelson, a Maryland-based neurologist and sleep specialist, has noted in a lecture that clinical experience is making the same mistake over and over again, with ever-increasing confidence. That said, the functional aspects of a sleep appliance are unable to be judged until the patient falls asleep and the bed partner provides feedback, the patient uses a home sleep monitor (e.g., pulse oximeter and snoring apps), or a follow-up sleep study is conducted. Snoring and sleep apnea are conditions that patients are generally unaware of because they are asleep. Dentists report that most patients who seek care do so because of bed partner disturbance or daytime sleepiness that affects quality of life.
How Does TAP Work?
Dr. Thornton’s TAP design is a simple, stainless steel or chromium cobalt single-point hinge mechanism on the patient’s midline. It is micro-adjustable in 0.25 mm increments, allowing for very fine adjustments. The hinge uses an expansion screw that can be accessed with a hex tool. Each TAP hinge is precision-fabricated from a dentist’s prescription using triple-laminated (TL) bonded flexible liner.
When delivered to the patient, the TAP appliance can be advanced by turning the screw to the right or reversed by turning the screw to the left. The hinge mechanism fits in the front of the mouth on top of the teeth. There is some tongue room taken up by the hinge; however, most patients adapt rapidly. Because the hinge holds the jaw from sliding back, patients cannot open their mouth without dislodging the upper or lower member. Most patients easily adapt to this characteristic.
Oral Appliance Therapy Side Effects
A known side effect of MAD therapy is temporary morning bite change. When the mandible is advanced for eight to 10 hours per night, some patients find that their teeth do no come back into occlusion right away. For this reason, an AM Aligner is included with every TAP appliance.

The TAP appliance is cleared by the FDA for the treatment of both snoring and obstructive sleep apnea. It has also been verified as Pricing, Data Analysis and Coding (PDAC) qualified for Medicare code E0486 for patients who are covered by Medicare.
Conclusion
The TAP appliance is a premium sleep therapy solution with a great track record and a clear treatment philosophy — and it leads the dental sleep industry in peer-reviewed literature. The lab process is well established, with New West Dental Ceramics offering a per-appliance delivery time of five days.
The patient record requirements use materials and techniques that are generally available in any non-specialty dental office. The most important feature of the TAP appliance is its titration element. The outcomes are better because patients own their condition and are responsible for monitoring their own symptoms under the guidance of a trained dentist. This is a model that works because the patients have the appropriate tool for success.
To learn more about sleep therapy, or to explore the New West family of sleep appliances, click here.


